EMBRYO DEVELOPMENT
Embryo development of human explained in four stages namely fertilization, pre-embryo development, embryo development and fetal development. The time of development is also called as gestation and lasts approximately 81/2 months. The gestation period commonly referred to as pregnancy.
1. FERTILIZATION:
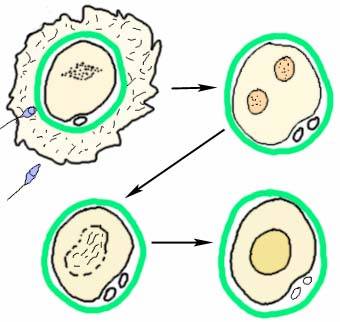
The penetration of the secondary oocyte by the sperm is called fertilization or conception. In the human, fertilization usually takes place in the uterine tube of the female. This penetration causes changes in the surface of the egg that allow no other sperm to enter and triggers the completion of meiosis. After the sperm sheds its tail, the nuclei of the egg and sperm fuse to form a zygote, the first cell of a new individual. With the union of the chromosomal material of both gametes, the zygote begins to divide by mitotic cell division.
2. PRE-EMBRYO DEVELOPMENT:
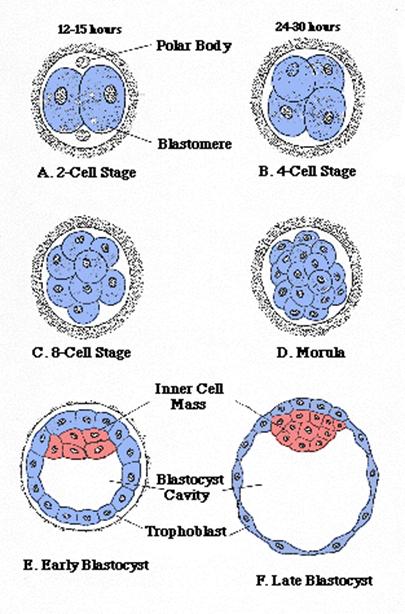
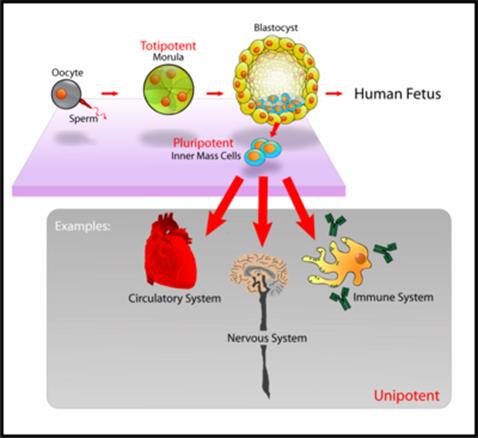
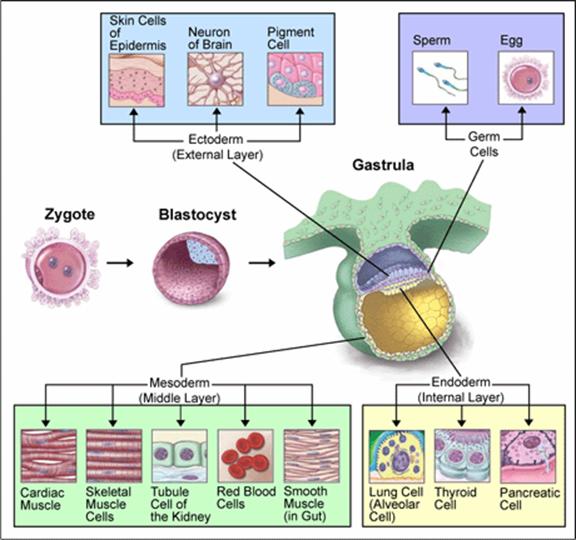
Within 30 hours, the one celled zygote begins to divide rapidly; one cell into two, two into four, four into eight, and so forth, producing a cluster of cells. This process of cell division occurs without cell growth and is called as cleavage. During this division process the cell-mass which is also called as pre-embryo move towards uterus. When the cell number is 16, the clustered cells called as morula, from a Latin word meaning “mulberry”. After 4 to 5 days in the uterus, the morula has developed into blastocyst. Cell migration, which begins to shape the pre-embryo, is the process that begins approximately 4 days after fertilization. Cell migration helps shape the developing individual in a process called morphogenesis. At this early stage, cell movement results in the formation of a hollow ball of cells known as a blastocyst in humans and in other mammals a stage more generally called the blastula. The center is filled with fluid from the uterine cavity. Like the term morula, the term blastocyst is descriptive, derived from two Greek words meaning “germ (germinal) sac”. One portion of the blastocyst contains a concentrated mass of cells destined to differentiate into the various body tissues of the new individual. It is referred to as inner cell mass. The outer ring of cells, called the trophoblast from a Greek word meaning “nutrition” will give rise to most of the extraembryonic membranes, including much of placenta, an organ that helps maintain the developing embryo.
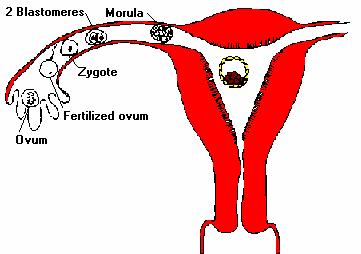
After the development of blastocyst, it secretes enzymes that digest a microscopic portion of the uterus. It then nestles into this site, nourished by the digested uterine cells, in a process called implantation. Blastocyst secretes Human chorionic gonadotropin (HCG). HCG acts on the corpus luteum in the ovary. The corpus luteum responds by continuing to produce estrogens and progesterone, hormones that sustain the implanted blastocyst as the placenta develops.
3. EMBRYO DEVELOPMENT (THREE TO EIGHT WEEKS):
During this crucial period, the developing individual is termed an embryo. Throughout the next six weeks, the embryo takes on a human shape by means of the ongoing process called morphogenesis. During morphogenesis, cells move to shape the developing embryo. In addition, the organs are established but need further development during the third through eight weeks in a process called organogenesis. Because of the incredible array of developmental processes proceeding simultaneously during this period, the embryo is particularly sensitive to teratogens, certain agents such as alcohol that can induce malformations in the rapidly developing tissues and organs.
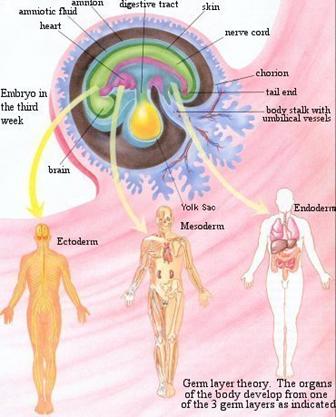
At the end of second week and continuing into the third week, various cell groups of the inner cell mass begin to divide, move and differentiate, changing the two layered pre-embryo into a three layered embryo. This process called as gastrulation. This process, in human as well as vertebrates, results in a developmental stage called the gastrula. The three primary germ layers are called ectoderm (‘outer skin’), endoderm (‘inside skin’) and the mesoderm (‘middle skin’). The endoderm produces tissue within the lungs, thyroid, and pancreas. The mesoderm aids in the production of cardiac muscle, skeletal muscle, smooth muscle, tissues within the kidneys, and red blood cells. The ectoderm produces tissues within the epidermis and aids in the formation of neurons within the brain, and melanocytes.
|
Germ Layer |
Category |
Product |
|
Endoderm |
General |
Gastrointestinal tract |
|
Endodern |
General |
Respiratory tract |
|
Endoderm |
General |
Endocrine glands and organs (liver and pancreas) |
|
Mesoderm |
General |
Bones |
|
Mesoderm |
General |
Most of the Circulatory system |
|
Mesoderm |
General |
Connective tissues of the gut and integuments |
|
Mesoderm |
General |
Excretory Tract |
|
Mesoderm |
General |
Mesenchyme |
|
Mesoderm |
General |
Mesothelium |
|
Mesoderm |
General |
Muscles |
|
Mesoderm |
General |
Peritoneum |
|
Mesoderm |
General |
Reproductive System |
|
Mesoderm |
General |
Urinary System |
|
Mesoderm |
Vertebrate |
Chordamesoderm |
|
Mesoderm |
Vertebrate |
Paraxial mesoderm |
|
Mesoderm |
Vertebrate |
Intermediate mesoderm |
|
Mesoderm |
Vertebrate |
Lateral plate mesoderm |
|
Ectoderm |
General |
Nervous system |
|
Ectoderm |
General |
Outer part of integument |
|
Ectoderm |
Vertebrate |
Skin (along with glands, hair, nails) |
|
Ectoderm |
Vertebrate |
Epithelium of the mouth and nasal cavity |
|
Ectoderm |
Vertebrate |
Lens and cornea of the eye |
|
Ectoderm |
Vertebrate |
Melanocytes |
|
Ectoderm |
Vertebrate |
Peripheral nervous system |
|
Ectoderm |
Vertebrate |
Facial cartilage |
|
Ectoderm |
Vertebrate |
Dentin (in teeth) |
|
Ectoderm |
Vertebrate |
Brain (rhombencephalon, mesencephalon and prosencephalon) |
|
Ectoderm |
Vertebrate |
Spinal cord and motor neurons |
|
Ectoderm |
Vertebrate |
Retina |
|
Ectoderm |
Vertebrate |
Posterior pituitary |
Organogenesis achieved mainly by the process of tissues differentiation. During tissue differentiation, groups of cells become distinguished from other groups of cells by the jobs they will perform in the body. This differentiation appears to be accomplished by the interaction of cytoplasmic stimulators and inhibitors of certain cells wih various genes of other cells. This process is induction. Because of these variation new organs emerged.
From the fourth to eighth weeks of development, dramatic changes takes place in the embryo. The embryo grows from a length of 2 millimeters to approximately 30 millimeters. A primitive circulation is established within the embryo, and a maternal-fetal exchange of nutrients, gases, and wastes begins. The central nervous system and its associated structures begin to develop. The body form is established, including the appendages.
HEART DEVELOPMENT
Development of the heart and vascular system begins very early in mesoderm both within (embryonic) and outside (extra embryonic) the embryo. Vascular development therefore occurs in many places, the most obvious though is the early forming heart, which grows rapidly creating an externally obvious cardiac "bulge" on the early embryo.

The heart forms initially in the embryonic disc as a simple paired tube inside the forming pericardial cavity, which when the disc folds, gets carried into the correct anatomical position in the chest cavity.
Embryological Timetable |
||||
|
Weeks |
Days |
Somites |
Length in mm |
Cardiac Events |
|
1-2 |
0-20 |
1 |
1.5 |
No heart or great vessels |
|
3 |
20 |
2 |
1.5 |
Cardiogenic plate |
|
3 |
21 |
5 |
1.5 |
Endocardial tubes |
|
4 |
22 |
10 |
2 |
Fusion of endocardial tubes |
|
4 |
23 |
12 |
2 |
Single median cardiac tube,first contraction ( ineffective) |
|
4 |
25 |
17 |
2.5 |
Cardiogenic loop |
|
4 |
26 |
20 |
3 |
Single atrium |
|
5 |
29 |
25 |
4 |
Bilobed atrium |
|
5 |
30 |
26 |
4 |
Beginning of circulation |
|
7 |
49 |
|
20 |
4-chambered heart, Absorption of pulmonary veins |
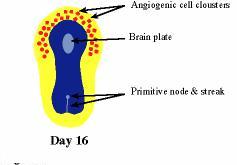
The first indication of heart development is around day 16-19. Clusters of angiogenetic cells form a "horseshoe-shaped" cluster anterior and lateral to the brain plate. The heart raises from a little group of special cells located in the embryological region which will become the chest. During the first four weeks of pregnancy this cells grow until they form a tube called the primitive heart tube.
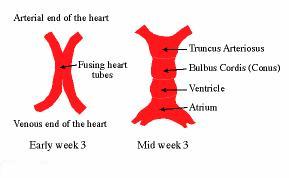
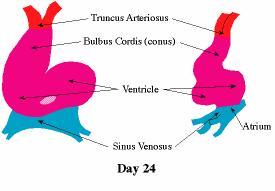
Following cardiac mesoderm involution during gastrulation, the two endocardial tubes fuse along the embryonic midline. The heart starts to beat at day 22, but the circulation does not start until days 27 to 29. The single tubular heart develops many constrictions outlining future structures. It is constituted of four segment: the seno-atrium which forms the atria, the primitive ventricle which forms the left ventricle, the heart bulb which forms the right ventricle and the truncus arteriosus which forms the aorta and the pulmonary artery. In the primitive heart tube the blood arrives in the senoatrium, travel through the tube and go out through the truncus arteriosus.
Prior to looping the heart tubes forms constrictions defining separate components of the heart, these are (cranial to caudal): Bulbus Cordis, Ventricle and Atrium. The primitive atrium is still paired and connects caudally to the paired sinus venosus. The heart tube will bend ventrally, caudally and slightly to the right.
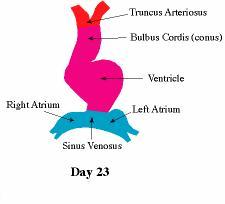
At this stage the paired sinus venosus extend laterally and give rise to the sinus horns. As the cardiac looping is developing the paired atria form a common chamber and move into the pericardial sac. During the next step the primitive heart tube coils up in a handle giving two atria and two ventricles. The right atrium connects to right ventricle through the tricuspid valve, left atrium connects to the left ventricle through the mitral valve. Contemporaneously are formed the atrial and the ventricular septum. The truncus arteriosus branches into aorta and pulmonary artery which connect respectively to the left and right ventricle. At ten weeks the heart is completely formed and functional and during the rest of the pregnancy it will grow to supply the demand of developing fetus.
Embryological development of the heart. A. Primitive heart tube stage. The senoatrium (SA) will give right and left atrium; the primitive ventricle (V) is the precursor of left ventricle; the bulbous cordis (BC) will give the right ventricle; the truncus arteriosus (TA) will branch into aorta (A) and pulmonary artery (P). B. C. D. Successive stages of the development up to an heart with 4 cavities.

A key aspect of heart development is the septation of the heart into separate chambers. As the embryonic/fetal circulation is different to the neonatal circulation (lung/pulmonary activation), several defects of heart septation may only become apparent on this transition. One septal "defect" occurs in us all, the foramen ovale (between the 2 atria) which in general closes in the neonate over time.
The peripheral vasculature can be thought of as 3 aortic/venous circulatory systems: placental (unbilical), embryonic and vitelline. The placental system develops mainly in the extraembryonic mesoderm of the chorion, receives maternal nutrition, removes embryonic waste and is lost with the placenta at birth. The vitelline system covers the surface of the yolk sac and contributes to the portal system (between gut and liver). The embryonic system begins symmetrically (L/R) within the embryo, and is extensively remodelled, in particular in the pharyngeal arches, to mature into our cardiovascular system.
Embryonic Heart Rate (EHR), early in development the heart starts to spontaneously beat and a recent study by Wisser and Dirschedl in dated human embryos showed an increase up to 63 postmenstrual days or 22 mm greatest length. Thereafter a steady decrease of EHR was noted. Maximal EHR is reached when morphological development of the embryonic heart is completed.
The human heart beats more than 3.5 billion times in an average lifetime. The human embryonic heart begins beating approximately 21 days after conception, or five weeks after the last normal menstrual period (LMP), which is the date normally used to date pregnancy. The human heart begins beating at a rate near the mother’s, about 75-80 beats per minute (BPM). The embryonic heart rate (EHR) then accelerates linearly for the first month of beating, peaking at 165-185 BPM during the early 7th week, (early 9th week after the LMP). This acceleration is approximately 3.3 BPM per day, or about 10 BPM every three days, an increase of 100 BPM in the first month.
After peaking at about 9.2 weeks after the LMP, it decelerates to about 150 BPM (+/-25 BPM) during the 15th week after the LMP. After the 15th week the deceleration slows reaching an average rate of about 145 (+/-25 BPM) BPM at term. The regression formula which describes this acceleration before the embryo reaches 25 mm in crown-rump length or 9.2 LMP weeks is:
Age in days = EHR(0.3)+6
There is no difference in male and female heart rates before birth
This period is primarily one of development. By the ninth week, most of the body systems are functional. The primary job of the fetal period is the refinement, maturation, and growth of these organ systems and of the body form of the developing individual. This period divided into three trimester periods namely first, second and third trimester with three months in each period including early weeks in first trimester. During third month (first trimester) the fetus grows to 3 1/3 inch in length. Eyes become well-developed and ears begin to form. During second trimester, the fetus grows to 30cm (12 inches) in length and begins to look human. The sensory organs become well developed and the bones begin to form, replacing cartilage. By the end of third trimester, the neurological growth of the fetus is far from complete and in fact, continues long after birth. By this time, the fetus is able to exist on its own.